Policy
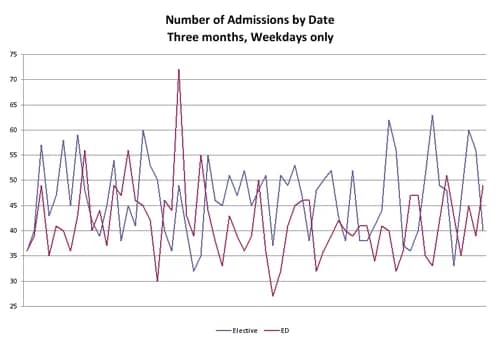
As someone with an interest in healthcare policy, you spend much energy trying to solve important issues such as the quality and safety of care delivery, emergency room overcrowding, nurse staffing, access to care and cost. One of the root causes of all of these challenges is artificial variability in the flow of certain (scheduled) types of patients through the care delivery system. Take, for example, the flow of elective (scheduled) and emergency admissions to a hospital. See one hospital’s experience over a three month period.